Incidence of
strabismus is 5-8% in the general population1. Typically, it encompasses
a deficiency of harmonization between the two eyes, which prevents the gaze of
each eye to the same point in space, thus inhibiting binocular vision and depth
perception2. Most common types of strabismus are ‘Exotropia’ and
‘Esotropia’. Exotropia is an outward deviation of the eye and usually starts at
the age of 2-4 years. Exotropia may be constant or intermittent where inward
deviation of one or both eyes occurs in esotropia. It can be constant or
intermittent. Ametropia indicates presence of a refractive error3,4.
The patient can get different ametropic conditions such as
hypermetropia, myopia or astigmatism. For instance, Myopia is a type of refractive error where parallel rays
of light coming from infinity are focused in front of retina when accommodation
is at rest.5In addition, hypermetropia is also called long sightedness
when parallel rays of light coming
from infinity are focused behind the retina with accommodation at rest. Astigmatism is a type of refractive error
where eye has different refractive powers in different meridians6-9.
A large numbers of heterotropic population have refractive errors,
which can positively or negatively affect the deviation. The main cause of the
refractive errors is heterotropia, which is the main interest of the study. We
carried out a perspective study to evaluate the association between refractive
errors and heterotropia.
MATERIAL AND METHODS
An
institutional based cross sectional data was collected from College of
Ophthalmology and Allied Vision sciences, Eye OPD pediatrics clinic Mayo
Hospital Lahore and a non-probability convenient sampling technique was used to
collect the data. A sample of 100 patients (October 2015 to December 2015) with
heterotropia up to the age of 40 years was examined for in the analysis. Data
was collected by clinical examination and the findings were recorded in a self-designed
proforma consisting of patient profile, strabismus history, visual acuity, motor
assessment and diagnosis.
Visual acuity of patients was observed using visual acuity chart (VLC)
monitor at distance and visual acuity of either eye was recorded in decimal notation.
Refractive error and orthoptic assessment of the patients was also recorded for
further analysis. Patients with cataracts, subnormal best-corrected visual
acuity, nystagmus and aphakics were excluded from the study. SPSS (version 16)
was used for statistical analysis and results.
RESULTS
There were
43% patients with emmetropia, 2% patients had myopia while 9% had hyperopia.
28% of the patients were having hyperopic astigmatism and 15% of the patients
were found with myopic astigmatism while 3% had mixed astigmatism (Fig. 1).
Hyperopia and
hyperopic astigmatism were more prevalent in esotropia whereas myopia, myopic
astigmatism and emmetropia were more common in exodeviations (Fig. 2). No
significant association between hypertropia and refractive errors was present.
Subsequently the amount of deviation at distance in most of the patients was
seen in the range of 26-45 prism diopter (PD), however 35% of patients showed
deviation of 5-25 PD, 15% illustrated 46-65 PD
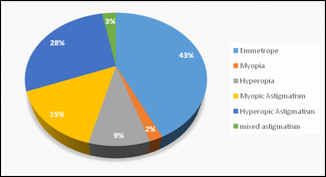
Fig. 1: Distribution of patients according to
Refractive Error.
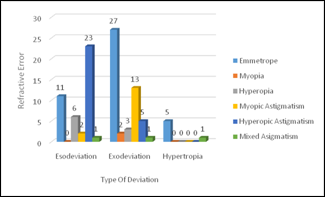
Fig. 2: Refractive Error and Type of Deviation.
and only 01% depicted 66-85 PD deviation. The distribution of
patients according to the amount of
deviation at near in majority of the patients lied in the range of 5-25
PD while 37% had 26-45 PD, 15% showed 46-65 PD, 5% showed 66-85 PD and 3% had
86-105 PD. A significant association between
refractive error and heterotropia was confirmed with (Chi-Square = 40.044, df =
10 and p = 0.000) as shown in Table 1.
DISCUSSION
The basic purpose
of this study was to counter check the association of refractive erorr with heterotropia.
The study was carried out at the Pediatric Eye Clinic Mayo Hospital
Lahore. World Health Organization has estimated that 153 million people
worldwide live with visual impairment due to uncorrected refractive errors10.
These anomalies of ocular alignment could have a
strong association with visual acuity, which is the reciprocal of the minimal resolvable visual angle measured
in minutes of arc for a standard test pattern11. In this study,
association between refractive error and misaligned eye was counter checked.
One hundred heterotropic patients aged between 4-40 years were included in the
study. Females were more than males with a male and female percentage of 42% and
58%.
Exotropia
commonly begins around age 2 to 4 years. It can appear at any age. Exotropia
may be constant or intermittent12-14.
Esotropia is a form of strabismus,
in which one or both eyes turn inwards. The condition can also be constant or
intermittent15. A study was
conducted in population-based sample and the
frequency of occurrence of ocular deviation and the carrier characteristics had
been identified. Despite other factors, the association of
the ocular deviation and refractive error, Esotropia
and also Exotropia can be present in individuals with varying degrees of myopia
(up to -5.75 for XT and -2.50 for ET) or hyperopia (up to +9.00 for XT and
+8.00 for ET)16.
A study concluded that strabismus was found in 45 of 170 children
(26.5%), and Esodeviation was the most common type. 9 (20%) had Exodeviation
and 4 (8.9%) vertical deviation. In 27 of 32 esotropic patients, the strabismus
was regarded as acquired esodeviations. The frequency of strabismus was lowest
in the high-grade hyperopia group (5%). Concerning esodeviations, fewer cases
(3%) were in the high-grade hyperopia group. Most of the cases with
esodeviations were in correlation with low-grade hyperopia (31%), myopia (28%)
and emmetropia (16%). Hyperopia was the most common refractive error.
Astigmatism was present in 72.4% of patients. Defocus in the peripheral retina
associated with the misalignment of the eyes during near work might be the
reason for the differences, considering the visual regulation mechanism of
eyeshape17, 18. Another, study revealed that in children with
intermittent exotropia, myopia was calculated to occur in more than 90% of
patients. Observation versus surgical correction did not alter the refractive
outcome19,20.
In our study emmetropic population was 43% (43), myopes 2% (2),
hypermetropes 9% (9) while myopic astigmatism was found in 15% (15), hypermetropic
astigmatism in 28% (28) and mixed astigmatism was 3% (3). The Amount of
deviation at distance and the number of patients in the range of 5-25 pd were
35% (35), in 26-45 pd were 49% (49) and in 46-65 pd were 15% (15) and in 66-85 pd
were 1% (1). A significant association between
refractive error and Heterotropia was found (Chi-Square 40.044) (p value 0.000).
62.8%
emmetropes had exotropia while 25.6% had esotropia and 11.6% were hypertropic.
All myopes in our study had Exotropia. In hyperopic patients, 66.7% had
Exotropia and 33.3% had Esotropia. 86.7% with myopic astigmatism had Exotropia,
13% had Esotropia. In hyperopic astigmatism,
17.9% had Exotropia and 82.1% had Esotropia. 33% of mixed astigmatic patient
had Exotropia, 33.3% had Esotropia and 33.3% had hypertropia. The limitation of
our study was that the data was collected from only one tertiary care center.
More studies are needed to find the situation across the country.
CONCLUSION
Our study confirmed
that heterotropia is strongly associated with refractive errors. It is observed
that hyperopia and hyperopic astigmatism was more prevalent in esotropia,
emmetropia, myopia. Myopic astigmatism was more common in exodeviations.
Author’s Affiliation
Dr. Syeda Rushda Zaidi
M. Phil, Orthoptist
College of
Ophthalmology and Allied Vision Sciences, King Edward Medical University,
Lahore
Dr. Mohammad Ali A Sadiq
FCPS, Assistant
Professor
College of
Ophthalmology and Allied Vision Sciences, King Edward Medical University,
Lahore
Dr. Asad Aslam Khan
FCPS, Professor
College of
Ophthalmology and Allied Vision Sciences, King Edward Medical University,
Lahore
Dr. Hijab Ijaz
Optometrist
DHQ Hospital Kasur
Role of Authors
Dr. Syeda Rushda Zaidi
Presented the main
idea, review of literature and data analysis.
Dr. Mohammad Ali A
Sadiq
Data collection and
analysis
Dr. Asad Aslam Khan
Overal guidance and
supervision.
Dr. Hijab Ijaz
Manuscript preparation.
REFRENCES
1.
Billson F.
Fundamentals of clinical ophthalmology. 1st ed. Malaysia. Elsevier,
2003: P.3.
2.
Louis S.
Optometric Clinical Practice Guideline: Care of the patient with strabismus:
esotropia and exotropia. American Optometric Association, 1997.
3.
Bhattacharyya, B.
Text book of visual science and clinical optometry. 1st edition. New
Delhi: Jaypee, 2009: p.118.
4.
Khurana AK.
Theory and practice of optics and refraction. 2nd edition. New
Delhi: Elsevier, 2009: p. 62.
5.
Elkington Frank JH, Greaney JM. Clinical optics. 3rd edition, 1999. (Optics of Ametropia;
Chap. 10): p.113-115.
6.
Bhattacharyya, B.
Text book of visual science and clinical optometry. 1st edition. New
Delhi: Jaypee, 2009: p. 120.
7.
Khurana AK.
Comprehensive Ophthalmology. 4th edition. New Delhi: New Age International (P)
Ltd. 2007: p.28.
8.
Khurana AK.
Theory and practice of optics and refraction. 2nd edition. New
Delhi: Elsevier, 2009: p. 79.
9.
Agarwal A. Agarwal S, Apple DJ, Burrato L, Alio JI, Pandy SK. Ophthalmology, 1ed ed. 2002; vol. 1: P.18.
10. Tanaka A, Ohno-Matsui K, Shimada N, Hayashi K, Shibata Y, Yoshida T et al. Prevalence of strabismus in patients with pathologic myopia. J Med Dent Sci. 2010 Mar; 57 (1): 75-82.
11. Rowe F. Clinical Orthoptics. 2nd ed. India: Blackwell publishing, 2004:p. 69-70.
12.
Rowe FJ.
Clinical Orthoptics. 3rd ed. UK. Wiley Black Well, 2012: p. 161.
13.
Clarke MP.
Intermittent exotropia. J of Pedriatr Ophthalmol & Strabismus, 2007
May/June; 44 (3): 153-157.
14.
Kanski JJ, Bowlding B. Clinical ophthalmology. 7th ed. USA. Elsevier, 2011.
Ch. 18. Strabismus: P. 771.
15.
Abrams.
Practice of refraction. 10 Edi. 2005: New Delhi: Blackwell, p. 37.
16.
Hyperopia. How
does the eye see? Available at URL http://www.laserlubbock.com/eye_basics.htm.cited
on 22/10/2010.
17.
Abrams.
Practice of refraction. 10 Edi. 2005. New Delhi. The refraction of the eye_
Physiological optics Chap. 3. p.47.
18.
Datta H. Strabismus.
1st ed. New Delhi: Jaypee, 2004: P. 31.
19.
Abrams.
Practice of refraction. 10 Edi. 2005. New Delhi. The refraction of the eye_
Physiological optics Chap. 3. p. 47.
20.
Datta H.
Strabismus.1sted. New Delhi: Jaypee, 2004: P. 31.